Occupational Lung Diseases: Causes, Consequences and Challenges
Ritwija Bhattacharya 1 , Anirban Biswas 2 , Sandip Bhattacharjee 3 and Pritha Bhattacharjee 1 *
http://dx.doi.org/10.12944/CWE.12.2.13
The systematic review synthesizes the diverse documentation of research on the burden of occupational lung disease (OLD) and its uncanny load in the modern industrial era greatly resembles iceberg phenomenon. The major OLDs include asbestosis, asthma, coal workers pneumoconiosis, chronic obstructive pulmonary diseases, hypoxia, lung cancer, metal fume fever, silicosis etc. We searched the literatures limited to English only in Pubmed, Scopus, Science Direct using selective keywords and cross references in different combinations. The search criteria retrieved relevant but highly scattered information or data on the present context spanning both global and Indian perspectives. The present review is an updated understanding along with retrospective data of the last twenty years. The main objective of the present review is to identify the causes of common lung diseases in different occupational sectors and their consequences. Conventional to alternative diagnostic methods and potential biomarkers for disease identifications have been summarized taking into account that early diagnosis of the disease has some limitations. Identification of the disease with early predictive biomarker will be challenging and may leave a foot print for greater societal benefit.
Copy the following to cite this article:
Bhattacharya R, Biswas A, Bhattacharjee S, Bhattacharjee P. Occupational Lung Diseases: Causes, Consequences and Challenges. Curr World Environ 2017;12(2). DOI:http://dx.doi.org/10.12944/CWE.12.2.13
Copy the following to cite this URL:
Bhattacharya R, Biswas A, Bhattacharjee S, Bhattacharjee P. Occupational Lung Diseases: Causes, Consequences and Challenges. Curr World Environ 2017;12(2). Available from: http://www.cwejournal.org/?p=17260
Download article (pdf) Citation Manager Publish History
Introduction
Lung diseases are the pinnacle of occupational diseases. Chronic exposure to irritants at work site can lead to pulmonary disease that may persist for prolonged period, even after the exposure ceases. Occupational lung diseases (OLDs) are a broad group of pulmonary diseases developing either from repeated or persistent inhalation of particulate matters, which causes morbidity and even mortality of the workers. The prevalence of OLDs are a major health issue in the workers exposed to hazardous substances (chemical, physical, biological agents) in their workplaces; which lead to progressive deterioration of lung function causing severe respiratory problems such as asthma, chronic obstructive pulmonary disease (COPD).1 The most common symptoms of lung diseases, regardless of the etiology are coughing, shortness of breath, chest pain and constrictiveness, abnormal breathing patterns though signs and symptoms of these diseases might vary with the individual’s susceptibility. The toxic chemical may have either local effect (contact site) or systemic effect or both. It is necessary to assess the relative risk for workers exposed to various agents in workplace and monitor the degrees of exposure. OLDs including cancer do have long latency periods and once the disease is diagnosed, limited choices remain for recovery. Moreover, even after cessation of exposure, chronically exposed workers continue to be at risk. However, disease can be preventable, if management options are timely undertaken.
United States Occupational Health and Safety Administration (USOSHA), [http://www.osha.gov/laws-regs.html] provides guidelines for Permissible Exposure Limits (PELs) in the workplace, based on an eight hour exposure time for a worker. Though such PELs for particular carcinogens/toxicants have been adopted long back, elusive implementation may have its root in limited awareness among the workers and authorities; untrustworthy poor databases in developing countries. Only 5-10% of workers in the developing nations and 20-50% of the developed, industrialized nations have access to proper occupational health care facilities [http,//www.wpro.who.int/topics/occupational_health/en/].
The objective of the present review is to understand the major causes and consequences of OLDs and identify the biomarkers associated with it. We have also addressed several challenges and conflicts, like health issues of the workers with economic loss of the organisations associated with that particular occupation, global and Indian contexts regarding the health outcomes of the workers. Strategies to provide logical dimensions towards mitigation policies are also touched upon.
Methods
We implemented an extensive database search depending using academic bibliographic databases, like PUBMED (http://www.ncbi.nlm.nih.gov/pubmed), SCIENCE DIRECT
(www.sciencedirect.com/), Web of Science (https://webofknowledge.com/), SCOPUS (www.scopus.com/), literature searches using Google Scholar and hand searches of the literatures and references of the publications. Searches were limited to English language articles published till December 2016, that provided us the information regarding OLD exposure scenario, health outcomes, conventional disease diagnosis along with molecular biomarker assisted diagnosis, several challenges in the national and global context and scope of mitigations.
Results and Discussions
Toxic exposure and lung related diseases
Broadly, the lung related diseases are caused by occupational exposure to metal fumes, particulate matters, volatile organic compounds, asbestos, silica etc.2 Diesel exhaust contains a number of gaseous and particulate chemicals that include soot and polycyclic aromatic hydrocarbons (PAH) along with other known carcinogens (American Cancer Society; https://www.cancer.org/ cancer/cancer-causes/diesel-exhaust-and-cancer.html). The home makers continuously exposed to biomass smoke for cooking and related purposes, sometimes suffer from COPD, bronchitis, tuberculosis and also lung cancer.3 Cleaning products that are hazardous to eyes, skin through contact and trachea through inhalation are widely used by the professional cleaners, it is a major public health issue as they represent a huge workforce.4 Literatures show significant proportion of workers exposed above PELs for silica,5-6 or benzene7 in developing countries like China or South Africa. Coal and asbestos miners, paper and pulp mill workers, agricultural workers, welders and those who are exposed to dust chronically, develop several lung related diseases associated with COPD, asthma, pulmonary fibrosis, pneumoconiosis, silicosis, plural malignant mesothelioma8-9 and other lung related diseases.
Asbestosis
Exposure to asbestos is associated with lung cancer and non-malignant respiratory diseases in asbestos miners. Prolonged exposure to asbestos is associated with diffused interstitial fibrosis in the workers.10 First reported from Spain in 1997, as occupational disease and the total identified cases were 16,463 among the social affiliated employees till 2011.11 In India, the workers employed in cement industry, the prevalence of asbestosis is 3% to 5%; while in US, about 9% in textile industry, 3% in mining and 21% in milling unit per year.12
Asthma
Asthma, a disease associated with the broncho-inflammatory response with symptoms like wheezing, coughing, chest constrictiveness and shortness of breath, may ultimately lead to reactive airways dysfunction syndrome. Most commonly found among the pulp and paper mill workers.8, 13 Literature revealed four most common chemicals associated with occupational asthma are mixture of chemicals (19.7%), cleaning materials (11.6%), mineral and inorganic dust (11.1%), and indoor pollutants (9.9%) [http://www.lungusa.org 1-800-LUNG-USA].
Coal worker's pneumoconiosis (CWP)
Also called ‘‘black lung disease’, which is an interstitial lung disease caused as a result of long-term exposure to coal dust and its accumulation in lung. The coal dust causes fibro-genetic reactions and black pigmentation of lung tissues.10 Symptoms including shortness of breath, deranged pulmonary function and often lung cancer are observed commonly in coal miners.14 As India is rich in mineral deposits, extensive coal mining opportunity along with prevalence of pneumoconiosis about 18.8% in India15 is noticed.
Chronic Obstructive Pulmonary Disease (COPD)
COPD is associated with chronic bronchitis and emphysema. It is a chronic lung disease. Most of the lung diseases are associated with COPD. It has occurred mainly as a result of exposure to hazardous vapour, gases, biological dusts, mineral dusts, organic dusts like wood, grains, diesel exhaust, metal fumes, and/or chemical gases or vapours when inhaled caused COPD or worsened the condition in workers who already have COPD.16,1 Some studies recommended that chronic exposure to silica dust does not cause disabling silicosis but surprisingly lead to the development of small airways disease or COPD which cause airflow obstruction.17
Hypoxia
High altitude workers are subjected to hypoxia which is seen in the mountaineers.18 Working for years at high altitude may accelerate the rate of decline of lung functions.19 Hypoxia is not only an exclusive problem for mountaineers only but also a problem in workers at mountain rescue services, in cable cars in ski areas and travelling businessmen.20
Lung cancer
Prolonged exposure to occupational carcinogens like asbestos, cadmium, chromium, diesel exhaust, silica and others that enter into the system through inhalation and further lead to multiple health problems including lung cancer. Workers exposed chronically to asbestos in their occupational setting, end up with bronchial carcinoma, pleural mesothelioma and cancer due to accumulation of asbestos fibres and asbestos bodies in their lung21 Sulphur dioxide exposure in workers of pulp and paper mills may lead to malignant pleural mesothelioma22 and continuous BTEX (benzene-toluene-ethylene and xylene) exposure in petrol pump workers and potash miners with exposure to chronic diesel motor exhausts may cause lung cancer.23-24
Metal fume fever
Exposure to metal fume particulate matters is very common in occupations like mine worker, welders, brass workers, transportations. Welding produces various contaminants small particles that upon vaporization rapidly condenses in air and are imperceptible in nature, but collectively, form a visible cloud. The fumes contain many chemicals like zinc oxide (ZnO) or magnesium oxide (MgO), fuming silver, gold, or platinum, cadmium, chromium and many more. The health effects vary according to specific metals present and duration of exposure ranging from short term illnesses, such as flu or long-term damage like lung cancer or neurological disease such as Parkinson’s disease.25 Amongst the welders, respiratory syndromes including asthma, metal fume fever are commonly reported.26
Silicosis
Exposures to large amounts of silica for short term or exposure lower levels of silica may cause silicosis [https://www.cdc.gov/niosh/docs/2015-106/]. It is the fibrotic disease of lungs with symptoms like gradually increasing dyspnoea and cough caused by inhaling fine particles of silica, in the form of cristobalite and quartz. Silica is widely used in industries including mining, manufacturing, foundries and construction related activities. Around 41,643 workers from industrial sectors of Italy were found to be at risk of silica exposure during 1996-2012, with characteristic risk from construction, mining and quarry sectors.27 Another study shows more than 3.2 million workers in the European Union had exposure to crystalline silica.28About 15.7% mining machine operators and about 9.5% non-construction manual workers died from silicosis exposure in US (http://www.lungusa.org 1-800-LUNG-USA). In India, it was mainly observed among the slate pencil cutters (54.6% prevalence) and stone quarry workers (22.4% prevalent), which is presumably under reported (http,//www.nioh.org).
Diagnosis of OLDs
Occupational exposure and subsequent health effects depend not only on the dose and nature (acute / chronic; single / multiple) of toxicants but also the individuals’ physical and physiological characteristics (age, sex, body weight, bio transformation capability, genetic make-up etc), which altogether play a pivotal role towards susceptibility. The effects can be further modulated due to concomitant exposure of other synergistic chemicals either from exposure sources or due to addiction towards tobacco, alcohol etc. In case of diseases like pneumoconiosis and silicosis, the patients don’t seek medical advice until those are complicated and worsened by bacterial infections like tuberculosis or extreme irritation from the exposure to intolerable dust and fume. Due to the lack of implementations of proper investigations and biological monitoring in most the cases, the diseases go undiagnosed at their initial stage and are detected at an advanced stage when only few options remain left for prevention. Diagnosis, treatment and prevention of diseases of occupational origin requires specific knowledge and experience that are not available adequately in most of the developing nations, is the main obstacle in data collection and health surveillance. Moreover, in countries like India, responsibility for health and safety at work is divided between labour and health ministries and this dual responsibility might lead to difficulty in data collection.29
Conventional methods
Herein, we will discuss the conventional strategies those are followed like Chest X rays, CT scan Pulmonary function tests, etc.30 Moreover, microscopic examination from biopsy or autopsy of tissue, cells, and fluids from the lungs are performed. It is also important to measure respiratory or gas exchange functions, airway obstructions and bronchial reactivity of the exposed individuals.31 Studies showed that nanoparticles may increase toxicity potential in comparison to the same material in the bulk form. A new method was developed to reveal asbestos nanofibers from tissues that were Formalin-Fixed Paraffin-Embedded (FFPE). Energy Dispersive X-ray (EDX) microanalysis was performed through transmission electron microscopy to express the occurrence of asbestos nanofibers in histological samples of patients with occupational exposure to asbestos.32
Alternative strategies and potential biomarkers
Alternative strategies including investigation of cellular and molecular changes are also immensely important for biomonitoring the exposed population. Several studies showed both chromosomal aberration and formation of micronuclei in peripheral blood lymphocyte predict genetic damage and instability. Asbestos exposure has been linked to pleural malignant mesothelioma, show elevated chromosomal aberration,33 micronuclei frequency, 34-35 and aberrant sister chromatid exchange. 36-37 However, Bolognesi et al., (2002)38 has observed no association of MN with asbestos exposure.
There are several studies, that attempted to identify molecular biomarkers for disease susceptibility among the chronic occupationally exposed populations (Table 1).
Table 1: Molecular biomarkers and the identification of the occupational lung diseases
|
Sl no. |
Molecular Biomarkers |
Identification of Diseases |
References |
|
1 |
Peroxiredoxins and tropomyosins as plasma biomarkers. |
Asbestos exposure, Lung cancer |
Rostila et al., 2012 |
|
2 |
Fibrulin 3 levels in blood in plasma and pleural effusions |
pleural mesothelioma as a result of asbestos exposure |
Pass et al., 2012 |
|
3 |
plasma FBLN-3 concentration |
exposure to carcinogenic fiber, fluoro-edenite malignant mesothelioma |
Rapisarda et al., 2015 |
|
4 |
Total lactate dehydrogenase (LDH) activity. |
Exposure to Silica |
Agarwal et al,,2014 |
|
5 |
Serum and urinary neopterin levels |
Silica exposure |
Altindag et al.,2003 |
|
6 |
serum levels of transforming growth factor-beta1 (TGF-β1), and MCP-1(monocyte chemotactic protein-1) |
Coal Workers Pneumoconiosis |
Lee et al., 2014 |
|
7 |
Elevated Ferritin and SOD in exhaled breath condensate (EBC) |
Non-small cell lung cancer |
Carpagnano et al., 2012 |
|
8 |
Development of 8-hydroxy-2'-deoxyguanosine (8-OHdG) within the DNA of white blood cells (WBC). |
Asbestos exposure and carcinogenicity |
Marczynski et al.,2000 |
|
9 |
8-nitroguanine(8-nitroG) is a mutagenic DNA lesion in human lung tissue |
Asbestos exposure and carcinogenicity |
Hiraku et al., 2014 |
|
10 |
angiogenic biomarkers, 80HdG and IL-6 mesothelin-related peptides(SMRPs) |
Asbestos exposure , malignant mesothelioma |
Amati et al.,2008 |
|
11 |
Reactive lipidp Peroxidase (LPO) and Reactive Oxygen Species(ROS), mRNA levels of tumor necrosis factor (TNF-α), interleukene-1β (IL-1β) and induction in micronuclei formation . |
Lung impairment and silicosis |
Ahmad et al., 2012 |
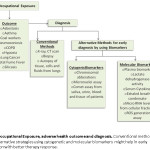
Serum cytokines like transforming growth factor-beta1 (TGF-β1), and MCP-1(monocyte chemotactic protein-1) was found to be elevated among progressive coal worker pneumoconiosis workers.39 Plasma peroxiredoxins 1 and 2, and tropomyosin 4 were found to be related to asbestos-exposure, and peroxiredoxin 1 to lung cancer.40 Plasma fibrulin 3 levels can differentiate a healthy person exposed to asbestos from that of a patient of mesothelioma as a result of exposure to asbestos. Plasma fibrulin 3 levels in combination with effusion can again distinguish mesothelioma effusion from other malignant and benign effusions.41 Correlation was found among plasma FBLN-3 concentration and pleural plaques in individuals exposed to carcinogenic fiber, fluoro-edenite. FBLN-3 has been anticipated as a biomarker for malignant mesothelioma as the plasma level of FBLN-3 showed awith high prognostic value.42 Plasma lactate dehydrogenase (LDH) activity was identified as an useful biomarker for silica exposure.43 In the individuals exposed to silica the alteration of neopterin was examined which is an early biomarker of cellular immunity. Serum and urinary neopterin was found to be elevated in silicosis patients44 and established its' potential as an early biomarker of cellular immunity, that can be easily measured by ELISA, spectrophotometry and/or HPLC methods. Elevated Ferritin and SOD was found in exhaled breath condensate (EBC) in non-small cell lung cancer, which plays a promising role as an outcome predictor for lung cancer monitoring patients.45 Inhalation of asbestos fibers can induce the development of 8-hydroxy-2'-deoxyguanosine (8-OHdG) within the DNA of white blood cells (WBC), indicating the carcinogenic potential.46 Additionally, it can induce mutagenic DNA lesion 8-nitroguanine(8-nitroG) in human lung tissue that may lead to lung cancer.47 Some angiogenic biomarkers, mesothelin-related peptides(SMRPs) were studied which showed the association with the increased exposure to asbestos and the mortality from malignant mesothelioma and lung cancer. Increased levels of 80HdG and IL-6 indicated a high level of SMRPs. The study revealed that the combination of some angiogenic biomarkers along with specific mesothelioma-biomarker like SMRPs could be utilized to monitor the health conditions of the workers who have a record of asbestos exposure.48 Though it was tried to develop the early biomarker for mesothelioma by using soluble mesothelin-related peptide (SMRP), the result did not support the usefulness of its early detection.49 In a study on the toxicological effects of granite dust particles, the authors demonstrated that nanoparticles caused oxidative stress, inflammatory response and genotoxicity, by nearly two fold of reactive Lipid Peroxidase (LPO) and Reactive Oxygen Species(ROS), mRNA levels of tumor necrosis factor (TNF-α), interleukene-1β (IL-1β) and induction in micronuclei formation.50 Researchers have identified several occupational disease markers but it seems to remain confined within the proposals only (Fig-1); direct applications of these methods on patients are lacking due to limited resources, lack of awareness, economic burdens and manipulations in the management sectors.
 |
|
The current review on OLDs has mainly highlighted the major causes and their adverse effect on health outcome, the diagnosis strategies considering both conventional and alternative one, using molecular biomarkers. Regular monitoring of workers’ health and the use of molecular biomarkers i.e the integrative knowledge might be more promising for early detection of the disease, compared to conventional strategy alone.
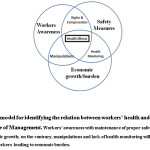
We have proposed a simple model showing the interactions among various factors that may impact on workers' health. Historical evidences show that often Management takes benefit over the general ignorance of the workers for their vested interest (Fig-2).
 |
|
A dark history was created by the MetLife (Metropolitan Life Insurance Company, US). The adverse effect of asbestos, silica were known to industries much before the public knowledge; however delayed scientific findings due to arbitrary manipulation, the problems got severe and unrecognized51. Canada, one of the major asbestos exporters targeted developing countries for the source of asbestos sales when the other industrialized countries after recognition of its hazardous health effects ceased to be their customers. Further awareness and enhanced collaboration among management team, occupational health experts and research scientists, could analyze the outcome in a holistic way to take the mitigation steps and right policy decisions for the benefit of workers.
Competing interest
The authors declare no competing interest of any financial benefit or other likely means. The authors also declare no conflict of interests as well.
Acknowledgement
Fund supported by National Tea Research Foundation (NTRF:175/2015) and University of Calcutta (BI:166/21) are highly acknowledged by the authors. AB acknowledges the research support through the NPDF, DST-SERB.
References
- Mazitova, N.N., Saveliev, A.A., Berheeva, Z.M., Amirov,N. K.,COPD and occupation, a retrospective cohort study of industrial workers. Archives of Industrial Hygiene and Toxicology, 63(3): 345-356(2012).
CrossRef - Bhattacharjee, P.1., Paul, S., Bhattacharjee, P., Risk of occupational exposure to asbestos, silicon and arsenic on pulmonary disorders: Understanding the genetic-epigenetic interplay and future prospects. Environmental Research, 425-34(2016)
CrossRef - Babalık, A., Bakırcı, N., Taylan, M., Bostan, L., Kızıltaş, S., Başbuğ, Y., Calışır, H.C., Biomass smoke exposure as a serious health hazard for women. Tuberkuloz Ve Toraks., 61(2): 115-121(2013).
CrossRef - Gerster, F.M., Vernez, D., Wild, P.P., Hopf, N.B.,Hazardous substances in frequently used professional cleaning products. International Journal of Occupational Environmental Health, 20(1), :46-60(2014).
CrossRef - Dosemecai, M., McLaughlin, J.K., Chen, J.Q., Hearl, F., Chen, R.G., McCawley,M.,Wu, Z., Peng, K.L., Chen, A.L., Rexing, S.H., Historical total and respirable silica dust exposure levels in mines and pottery factories in China. Scand. Journal of Work Environment and Health, 2, 39-43(1995).
- Rees, D., Cronje, R., duToit, R.S. Dust exposure and pneumoconiosis in a South African pottery. Study objectives and dust exposure. British Journal of Industrial Medicine., 49(7):44-464(1992).
CrossRef - Yin, S.N., Li, Q., Liu, Y., Tian, F., Du, C., Jin, C.,Occupational exposure to benzene in China. British Journal of Industrial Medicine,44(3):192–195(1987).
CrossRef - Murgia, N., Torén, K., Kim, .J.L, Andersson, E.Risk factors for respiratory work disability in a cohort of pulp mill workers exposed to irritant gases. BMC Public Health, 11(689), DOI,10.1186/1471-2458-11-689(2011)
- Mukherjee AK, Bhattacharya SK, Saiyed HN. Assessment of respirable dust and its free silica contents in different Indian coal minesIndustrial Health, 2005;43:277-284.
- Winder C and Neil S, Occupational Toxicology.2nd ed.CRC PRESS Boca Raton London New York Washington, D.C. 2003.
- Gomez TE, Rodriguez-Sanchez J, Diaz-Perales A et al. Occupational allergic multiorgan disease induced by wheat flour. J Allergy Clinical Immunology 2015;136:1114-1116.
CrossRef - World Health Organization. (2014). Chrysotile asbestos. Geneva 27, Switzerland. pp 1-52.
- Glindmeyer, H.W., Lefante, J.J., Freyder, L.M., Friedman, M., Weill, H., Jones, R.N. Relationship of asthma to irritant gas exposures in pulp and paper mills. Respiratory Medicine, 97(50), 541-548(2003).
CrossRef - Graber, J. M., Stayner, L. T., Cohen, R. A., Conroy, L. M., Attfield, M. D. Respiratory disease mortality among US coal miners; results after 37 years of follow-up.Occupational and Environmental Medicine, 71(10), 30-39(2014).
CrossRef - International Labour Organisation, (2013). ISBN 978-92-2-127446-9
- Mehta AJ, Miedinger D, Keidel D et al. Occupational exposure to dusts, gases, and fumes and incidence of chronic obstructive pulmonary disease in the Swiss cohort study on air pollution and lung and heart diseases in adults. American Journal of Respiratory and Critical Care Medicine 2012;185:1-1300.
CrossRef - Hnizdo, E., Vallyathan, V. Chronic obstructive pulmonary disease due to occupational exposure to silica dust, a review of epidemiological and pathological evidence. Occupational and Environmental Medicine, 60(4), 237-243(2003).
CrossRef - Powell, F.L., Garcia, N. Physiological effects of intermittent hypoxia. High. Alt. Med. Biol. 1(2), 125-136(2000).
CrossRef - Vinnikov, D., Brimkulov, N., Redding-Jones, R.Four-year prospective study of lung function in workers in a high altitude (4000 m) mine. High Altitude Medical Biology, 12(1), 65-69(2011).
CrossRef - Hillebrandt D., Milledge J., Kupper T. Occupational aspects of work in hypoxic conditions - the new recommendation of the medical commission of the union. Internationale des associations dalpinisme. Sports Medicine, Versita, Warsaw, 2010, 34-39(2010).
- Järvholm, B., Aström, E. The risk of lung cancer after cessation of asbestos exposure in construction workers using pleural malignant mesothelioma as a marker of exposure. J. Occupational Environmental Medicine, 56(12), 1297-1301(2014).
CrossRef - Fisher, R.P., Easty, D.B. Results of surveys at United States pulp and paper mills for the presence of scales and precipitates containing naturally occurring radioactive material (NORM). Health Phys.,84(4),518-525(2003).
CrossRef - Mohner, M., Kersten, N., Gellissen, J. Diesel motor exhaust and lung cancer mortality, reanalysis of a cohort study in potash miners. EuropianJournal of Epidemiology, 28(2), 158-168(2013).
CrossRef - Kendzia, B., Behrens, T., Jöckel, K.H., Siemiatycki, J., Kromhout, H., Vermeulen, R., Peters, S., VanGelder, R., Olsson, A., Brüske, I., Wichmann, H.E., Stücker, I., Guida, F., Tardón, A., Merletti, F., Mirabelli, D., Richiardi, L., Pohlabeln, H., Ahrens, W., Landi, M.T., Caporaso, N., Consonni, D., Zaridze, D., Szeszenia-Dabrowska, N., Lissowska, J., Gustavsson, P., Marcus, M., Fabianova, E., Mannetje, A., Pearce, N., Tse, L.A., Yu, I.T., Rudnai, P., Bencko,V., Janout, V., Mates, D., Foretova, L., Forastiere, F., McLaughlin, J., Demers, P., Bueno-de-Mesquita, B., Boffetta, P., Schüz, J., Straif, K., Pesch, B., Brüning, T.(2013Welding and lung cancer in a pooled analysis of case-control studies. Am J Epidemiol 2013;178:10.
CrossRef - Spear JE. 2004. Welding fume and gas exposure. CSP, CIH, Spear Consulting, LLC. Standard for exposure to asbestos dust, hearing before A.M. Goldberg. US Department of Labor (14–17 March 1972).
- El-Zein, M., Malo, J.L., Infante-Rivard, C., Gautrin, D. Prevalence and association of welding related systemic and respiratory symptoms in welders. Occupational Environmental Medicine 60(9), 655-661(2003).
CrossRef - Scarselli, A., Corfiati, M., Marzio, D.D., Iavicoli, S.Evaluation of workplace exposure to respirable crystalline silica in Italy. Int. J. Occupational Environmental Health,20(4), 301-307(2014)
CrossRef - Kauppinen, T., Toikkanen, J., Pedersen, D., Young, R., Ahrens, W., Boffetta, P. Occupational exposure to carcinogens in the European Union. Occupational Environmental Medicine, 57, 10–18 (2000).
CrossRef - Wong, J., Magun, B.E., Wood, L.J. Lung inflammation caused by inhaled toxicants, a review. Int. J. Chron. Obstruct. Pulmonary Disease, 11, 1391-1401(2016).
CrossRef - Ranu, H., Wilde, M., Madden, B. Pulmonary Function Tests. Ulster. Med. Journal, 80(2), 84–90(2011).
- Sharp, C.R., Rozanski, E.A. Physical examination of the respiratory system. Top Companion Anim Med., 28(3), 79-85(2013).
CrossRef - Scimeca, M., Pietroiusti, A., Milano, F., Anemona, L., Orlandi, A., Marsella, L.T., Bonanno, E.(2016). Elemental analysis of histological specimens, a method to unmask nano asbestos fibers. Eur J Histochem.2573(2016).
CrossRef - Ruosaari, S.T., Nymark, P.E., Aavikko, M.M., Kettunen, E., Knuutila, S., Hollmén, J., Norppa, H., Anttila, S.L. Aberrations of chromosome 19 in asbestos-associated lung cancer and in asbestos-induced micronuclei of bronchial epithelial cells in vitro. Carcinogenesis, 29(5), 13-17(2008).
CrossRef - Gövercin, M., Tomatır, A.G., Evyapan, F., Acikbas, Ä°., CoÅŸkun, G., Akdag, B. Elevated micronucleus frequencies in patients with pleural plaque secondary to environmental exposure to asbestos. Genetics and Molecular Research,13(1), 598-604(2014).
CrossRef - Marini, V., Michelazzi, L., Cioé, A., Fucile, C., Spigno, F., Robbiano, L., Exposure to asbestos, correlation between blood levels of mesothelin and frequency of micronuclei in peripheral blood lymphocytes. Mutat. Res., 721(1), 114-117(2011).
CrossRef - Fatma, N., Jain, A.K., Rahman, Q., Frequency of sister chromatid exchange and chromosomal aberrations in asbestos cement workers. Br. J. Ind. Med, 48(2),103-105(1991).
CrossRef - Atalay, F., Baltaci, V., Alpas, I., Savas, I., Atikcan, S., Balci, S., Sister chromatid exchange rate from pleural fluid cells in patients with malignant mesothelioma. Mutation Research, 465 (1-2), 158-163(2000).
CrossRef - Bolognesi, C., Filiberti, R., Neri, M., Perrone, E., Landini, E., Canessa, P.A., Simonassi, C., Cerrano, P.G., Mutti, L., Puntoni, R., High frequency of micronuclei in peripheral blood lymphocytes as index of susceptibility to pleural malignant mesothelioma. Cancer Research, 62(19), 5418-5419(2000).
- Lee, J.S., Shin, J.H., Lee, K.M., Hwang, J.H., Baek, J.E., Kim, J.H., Choi, B.S., Serum levels of TGF-β1 and MCP-1 as biomarkers for progressive coal workers' pneumoconiosis in retired coal workers, a three-year follow-up study. Industrial Health, 52(2), 129-136(2014).
CrossRef - Rostila, A., Puustinen, A., Toljamo, T., Vuopala, K., Lindström, I., Nyman, T.A., Oksa, P., Vehmas, T., Anttila, S.L., Peroxiredoxins and tropomyosins as plasma biomarkers for lung cancer and asbestos exposure.LungCancer, 77(2), 450-457(2012).
CrossRef - Pass, H.I., Levin, S.M., Harbut, M.R., Melamed, J., Chiriboga, L., Donington, J., Huflejt, M., Carbone, M., Chia, D., Goodglick, L., Goodman, G.E., Thornquist, M.D., Liu, G., de Perrot, M., Tsao, M.S., Goparaju, C., Fibulin-3 as a blood and effusion biomarker for pleural mesothelioma. N. Engl. J. Med., 367(15), 1417-1427(2012).
CrossRef - Rapisarda, V1., Ledda, C1., Migliore, M2., Salemi, R3., Musumeci, A4., Bracci, M5., Marconi , A1., Loreto, C6., Libra, M3., FBLN-3 as a biomarker of pleural plaques in workers occupationally exposed to carcinogenic fibers: a pilot study. Future Oncol.;11:35-7(2015).
CrossRef - Agarwal, B.D. Lactate dehydrogenase as a biomarker for silica exposure-induced toxicity in agate workers. Occupational and Environmental Medicine, 71(8), 578-582(2014).
CrossRef - Altindag ZZ1, Baydar T, Isimer A, Sahin G. Neopterin as a new biomarker for the evaluation of occupational exposure to silica. Int Arch Occup Environ Health.76(4):318-22. (2003).
- Carpagnano, G. E., Lacedonia, D., Palladino, G.P., Koutelou, A., Martinelli, D., Orlando, S., Foschino-Barbaro, M.P. Could exhaled ferritin and SOD be used as markers for lung cancer and prognosis prediction purposes? European Journal of Clinical Investigation, 42(5), 478-486(2012).
CrossRef - Marczynski B1, Rozynek P, Kraus T, Schlösser S, Raithel HJ, Baur X
- Hiraku, Y1., Sakai, K., Shibata, E., Kamijima, M., Hisanaga, N., Ma, N., Kawanishi, S., Murata, M., Formation of the nitrative DNA lesion 8-nitroguanine is associated with asbestos contents in human lung tissues: a pilot study. Occup Health;56(3):186-96(2014).
CrossRef - Amati M1, Tomasetti M, Mariotti L, Tarquini LM, Valentino M, Santarelli L. Assessment of biomarkers in asbestos-exposed workers as indicators of cancer risk. Mutat Res.655:52-8(2008)
CrossRef - Filiberti, R., Marroni, P., Spigno, F., Merlo, D.F., Mortara, V., Caruso, P., Cioè, A., Michelazzi, L., Bruzzone, A., Bobbio, B., Simonassi, C., DelCorso, L., Galli, R., Racchi ,O., Dini, G., Linares, R. .Is soluble mesothelin-related protein an upfront predictive marker of pleural mesothelioma? A prospective study on Italian workers exposed to asbestos. Oncology, 86, 33-43(2014).
CrossRef - Ahmad, I., Khan, M.I., Patil, G., Chauhan, L.K. Evaluation of cytotoxic, genotoxic and inflammatory responses of micro- and nano-particles of granite on human lung fibroblast cell IMR-90.Toxicology Letters,208(3), 300-307(2012).
CrossRef - Egilman, D.S., Bird, T., Lee, C. Met Life and its corporate allies, dust diseases and the manipulation of science. International Journal of Occupational Environmental Health, 19(4), 287-303(2013).
CrossRef








